

For four decades, the causal link between RAS mutations in cancer – including the KRAS, HRAS, and NRAS genes – has been well-accepted. But for almost as long, oncology drug development has struggled to develop RAS inhibitors, and many had long considered RAS an ‘undruggable’ target.1 With two recent landmark drug approvals erasing the ‘undruggable’ monicker and large government-, academic-, and industry-wide initiatives leading the attack on RAS, preclinical and clinical teams are focused now more than ever on developing novel RAS-targeted cancer therapies and treatment strategies.
Let’s look at RAS-driven oncogenesis and the past, present, and future of RAS drug development.
Oncogenic RAS Mutations in Cancer: KRAS, NRAS, and HRAS
According to large-scale genetics studies (e.g., MSK-IMPACT and AACR Project GENIE), variants in one of the three RAS genes (e.g., the human genes KRAS, NRAS, and HRAS) are the most common oncogenic mutations present in 20% of all cancers.2-4 That results in about 3.4 million new RAS-driven cancer cases annually around the globe.5
In certain types of cancer, RAS mutations are far more common. In pancreatic cancer, for instance, 90% of tumors have KRAS mutations, while 50% of colorectal cancer tumors have KRAS mutations. Across all solid cancers, 17% of all tumors have a KRAS mutation.
The other RAS oncogenes, NRAS and HRAS, are more common than KRAS mutations in different types of cancer. NRAS mutations are most prevalent in melanoma and hematological malignancies, whereas HRAS mutations occur more commonly in bladder, salivary gland, and head and neck cancers.2,3 This finding is consistent with previous research demonstrating that KRAS, NRAS, and HRAS play distinct cellular roles: Each has unique subcellular localizations, processing/trafficking, and phenotypes in individual RAS knockout mice.6-8
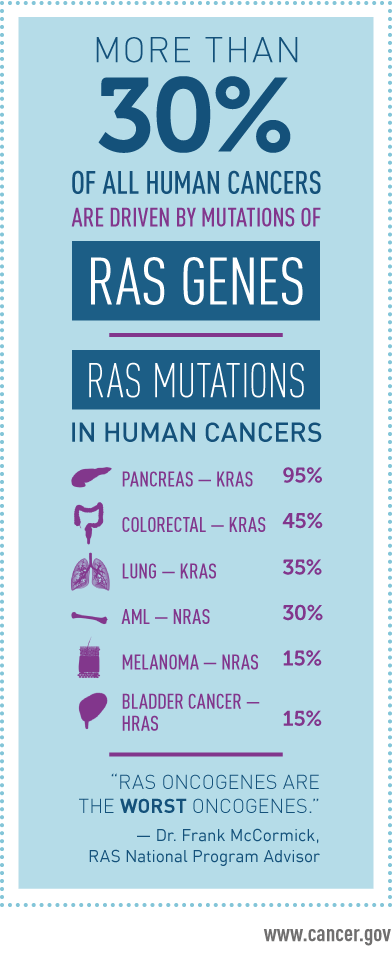
Figure 1: RAS Mutations in Human Cancers. More than 30 percent of all human cancers – including 95 percent of pancreatic cancers and 45 percent of colorectal cancers — are driven by mutations of the RAS family of genes. Source: National Cancer Institute (NCI). Dec. 2, 2014.
The Basics of RAS Function and its Role in Cancer
The RAS family of proteins are small GTPases that act as GDP/GTP-regulated switches that respond to various extracellular signals, including growth factors, cytokines, immunological pathways, and more. Accordingly, they influence key cellular decisions – proliferation, apoptosis, differentiation, and migration – as part of the MAPK and mTOR signaling pathways.9
KRAS, NRAS, and HRAS behave as prototypical GTPases.10 They are inactive when GDP is bound and active when GTP is bound. This activation switch is stimulated by RAS-guanine nucleotide exchange factors (RAS-GEFs), inducing an exchange of GDP for GTP. RAS-GTPase-activating proteins (RAS-GAPs) accelerate GTPase activity, leading to GTP hydrolysis and inactivation of RAS proteins. This cycle of activation and inactivation is accompanied by well-understood conformational changes in 2 domains, called switch 1 and switch 2.11
RAS activity is carefully controlled in healthy cells, and mutations can lead to dysregulation of the RAS signaling pathway in cancer. The most common RAS mutations in the G12, G13, or Q61 residue of KRAS, NRAS, or HRAS lead to constitutive activation, though the mechanism is different depending on the nature of the mutation.12 For example, KRAS G12C mutants have greater GTPase activity than other KRAS variants, though much reduced compared to wild-type KRAS. KRAS G12C mutants are also refractory to the activity of RAS-GAPs.13 Other KRAS mutants, such as KRAS Q61L and Q61H, can be activated by RAS-GAPs yet have very low GTPase activity.14
Ultimately, RAS overactivation leads to hyperactive downstream signaling cascades and increased activation of proliferative pathways. This drives increased cell division, growth, survival, and other hallmarks of cancer, including metabolic reprogramming and angiogenesis.15

Figure 2: RAS Pathway in Cancer. This diagram demonstrates (1) the upstream activators of RAS signaling, (2) regulators of RAS membrane localization, (3) regulators of RAS activity, (4) downstream signaling effector pathways, and (5) downstream functional effects of RAS signaling in cancers. Source: Front Oncol. 2019; 9: 965.
Drug Development Efforts Targeting the RAS Family
The decades-long search for small molecules that target RAS proteins has focused on drugging KRAS due to the grand size of the patient population it affects. However, several fundamental biochemical barriers have made drug development efforts for KRAS (as well as other RAS proteins) difficult.
First, and perhaps most important, there are few potential small-molecule binding sites, making it challenging to use structural data and rationally designed small molecules to generate promising candidates. Second, the binding pockets that do exist on RAS proteins have a picomolar affinity for GDP and GTP. Finally, the intracellular concentration of GTP is 500nM, which adds to the impact of the previous drug development difficulty.16
Taken together, this makes it nearly impossible to develop small molecules with binding affinities and intracellular concentrations that could outcompete the binding of GTP.17 On top of this, the diversity of KRAS mutations in the GTP/GDP binding pocket is high, leaving an increased potential for resistance.
Oncology drug development has taken other paths to get around these challenges, targeting upstream and downstream processes involved in RAS post-translational modification or signal transduction pathways.
Inhibition of RAS Membrane Association
RAS proteins undergo post-translational modifications that result in farnesylation of a C-terminal cysteine residue. Farnesylated RAS then inserts into the intracellular leaflet of the cell membrane. The first step in RAS farnesylation is catalyzed by farnesyltransferase (FTase), and RAS drug development efforts have focused on inhibiting this enzyme.
Early studies demonstrated that KRAS and NRAS-associated cancers were refractory to FTase inhibitors due to compensatory post-translational modification by other enzymes.18 While FTase inhibitors remain promising for HRAS-associated cancers, their low frequency and dubious role in driving tumorigenesis have made them less attractive for drug development. For KRAS and NRAS-driven cancers, combinatorial treatments of FTase and other inhibitors may hold promise, but development has stalled due to safety concerns.19 The enzymes involved in another lipid modification of RAS – palmitoylation – have also been a target of drug developers; however, a safe and effective drug would only apply to a small number of patients with KRAS-driven cancers.20
Inhibition of RAS-Mediated Signaling
RAS proteins are a key component of the RAF-MEK-ERK pathway. Signaling through this pathway is initiated through activation of receptor tyrosine kinases by growth factor, cytokine, or other binding events at the cell surface. Not surprisingly, drug developers have focused on targeting the members of this signaling pathway to mitigate the effects of RAS mutations that lead to increased signaling.
Many RAF inhibitors have been investigated; several are FDA-approved for indications such as BRAF mutation-driven melanoma. Paradoxically, these compounds activate downstream ERK-dependent signaling in RAS-driven cancers (though the mechanism of how this occurs is not fully understood).21
MEK and ERK inhibitors have also been extensively studied, and several compounds are FDA-approved for BRAF mutation-driven non-small cell lung cancer (NSCLC) and melanoma. MEK inhibitors have proven ineffective in RAS-driven cancers due to compensatory upregulation of receptor tyrosine kinases.22 Similarly, treatment with ERK inhibitors leads to increased MEK activation as ERK is involved in a negative feedback mechanism that leads to the inactivation of RAF.
Inhibition of RAS Directly
For the abovementioned reasons, targeting RAS proteins with small molecules is exceptionally challenging. The first inhibitors described competed with GDP binding, yet all the compounds studied were low potency and not ideal for drug development.23
Another class of RAS inhibitors that prevents RAS and RAF association, thus inhibiting downstream signaling, has also been investigated.24 Again, the major problem with these inhibitors was potency, and they stalled in pre-clinical development.
A Successful Step Forward: Drugging RAS Mutants
Despite these many therapeutic approaches, there has been one major breakthrough in RAS druggability: Targeting mutant forms of RAS. In 2013, inhibitors of KRAS G12C mutants were discovered from a screen of nearly 500 compounds.25
The lead compound was specific for the G12C mutant and was found to bind to GDP-bound KRAS G12C. Targeting mutant KRAS offers additional safety benefits because it has a lower risk of off-tumor (e.g., it can’t bind to wild-type KRAS or target non-malignant cells) and off-target effects. This initial discovery, additional medicinal chemistry efforts, and pre-clinical and clinical testing led to the development and approval of two KRAS G12C mutant-specific inhibitors, sotorasib (in 2021) and adagrasib (in 2022), for the treatment of NSCLC.26,27
The RAS Resistance Problem
These recent successes are a significant step forward for drugging RAS proteins. Yet, the current clinical data suggests modest efficacy. Sotorasib, for instance, exhibits an overall response rate of 41% and a median progression-free survival of only 6.3 months.28 In addition, patients can become resistant to KRAS G12C-specific inhibitors through several interrelated mechanisms.
Primary resistance due to pre-treatment mutational heterogeneity plays a minor role and large-scale sequencing efforts have found other non-G12C KRAS mutations in a small percentage of patients.29,30 Acquired post-treatment resistance plays a much larger role: Mutations in amino acid residues 12, 68, 95, and 96, which all form the binding site for sotorasib and adagrasib, can lead to resistance to one or both compounds.31 Other acquired mutations in NRAS, BRAF, and several other genes have been shown to confer resistance to KRAS G12C-specific inhibition.30 There are also additional adaptive mechanisms, such as reactivation of the RAF-MEK-ERK pathway, that play a role in resistance.32
Thus, significant drug development is still needed to address common resistance mechanisms and design novel strategies for RAS-driven cancers.
The Future Landscape of RAS Drug Development
Combination Therapies
Several combination therapies are under clinical investigation to address some of the common pathways to resistance. In NSCLC and colorectal cancer patients, a common adaptive mechanism to sotorasib and adagrasib treatment is the buildup of activated EGFR, a tyrosine receptor kinase involved in initiating activation of the RAS-Raf-MEK-ERK pathway.33,34 Accordingly, combination treatments of EGFR tyrosine kinase inhibitor afatinib with sotorasib are being investigated in NSCLC patients with KRAS G12C mutations, and recent readouts suggest a promising safety profile and modest improvements in efficacy.35 The anti-EGFR antibody, cetuximab, treatment has also been combined with adagrasib to test the safety and efficacy of this combination.
An upstream regulator of the RAS signaling pathway in cancer (though downstream of EGFR activation), SHP-2, drives RAS-GDP exchange for GTP, and several KRAS mutant NSCLC models are dependent on SHP-2 for growth.36 Therefore, it has become a promising target for combination strategies and trials that combine SHP2 inhibitors with adagrasib or sotorasib, which are currently testing the safety and efficacy in several KRAS mutation-driven solid tumors. Preclinical studies with SHP2 and KRAS G12C co-inhibition have emphasized investigating the tumor microenvironment (TME). A recent study by Fedele et al. demonstrated that more robust cytotoxic T-cell infiltration and anti-tumor response was observed in subcutaneous syngeneic KRAS G12C pancreatic ductal adenocarcinoma (PDAC) models treated with SHP2 and KRAS G12C inhibitors, compared to orthotopic models.13
Another axis of investigation for synergistic inhibitors is focused on targeting parallel signaling pathways outside of RAS-RAF-MEK-ERK. In pre-clinical studies, cyclin-dependent kinase 4/6 (CDK4/6) and KRAS G12C co-inhibition act synergistically in NSCLC and PDAC models.37 Targets such as mTOR complex 1/2 (mTORC1/2), which has increased activation during mutant KRAS inhibition and plays a role in adaptive resistance, and Aurora kinases, which are upregulated in mutant KRAS NSCLC cells and sotorasib-resistance cell lines, are also being investigated.38,39
Immunotherapies and The Tumor Microenvironment (TME)
KRAS mutations in cancer help to shape an immunosuppressive TME through the recruitment and activation of macrophages, suppression of cytotoxic T-cells, and activation of regulatory T-cells.40

Figure 3: The RAS Pathway Shapes Interactions Between Cancer Cells and the Immune Microenvironment. This diagram depicts mechanisms by which RAS signaling promotes cancer through (1) supporting cancer cell immune evasion and (2) driving immune-mediated stimulation of cancer cell growth. Source: Front Oncol. 2019; 9: 965.
A recent study by Tang et al., points to SHP2 as critical for establishing the KRAS mutant-driven immunosuppressive environment, as it can be mitigated by SHP2 inhibition in PDAC and NSCLC models.41
The immunosuppressive TME opens up the possibility of sotorasib or adagrasib augmenting the efficacy of immune checkpoint inhibitors that target PD-1, PD-L1, or CTLA4. Accordingly, synergistic tumor shrinkage and pro-inflammatory response were seen in mouse models co-treated with immune checkpoint inhibitors and sotorasib.42 Similar responses were seen in KRAS G12C xenograft models co-treated with an anti-PD-1 monoclonal antibody and adagrasib.43 While these pre-clinical studies were done using subcutaneous xenograft models and clinical applicability may be dubious, these combinations are currently being tested in several multi-arm phase I/II studies.
KRAS-on and pan-KRAS Inhibitors
Currently approved KRAS mutant therapies, adagrasib and sotorasib, are KRAS-off inhibitors, as they bind to mutant KRAS in their GDP-bound state. Drug development efforts have begun to focus on inhibiting RAS in the GTP-bound state, called KRAS-on inhibitors. Recent work has focused on targeting KRAS G12D as it has less GTPase activity than KRAS G12C. Cyclic peptides and non-covalent inhibitors that target the GTP-bound KRAS G12D have been identified and show promising pre-clinical data.44,45 They both bind in the switch 2 region.
Another promising treatment strategy has focused on inducing the formation of a trimeric complex consisting of compounds such as RM-018, a chaperone protein, cyclophin A, and GTP-bound mutant KRAS.46 Pan-KRAS-mutant inhibitors are in pre-clinical development using this same strategy with activity against some of the most common KRAS mutations in cancer, including G12D, G12V, and G12R in a PDAC model.47
Inducing RAS Degradation
The use of proteolysis-targeting chimera (PROTAC) technology for triggering the degradation of mutant KRAS is a promising new treatment modality for targeting RAS.48 PROTAC molecules are bifunctional and bring a target protein close to a ubiquitin ligase. Subsequent ubiquitination of the target and recognition by the cell’s proteolytic machinery leads to target degradation. Adagrasib and pan-KRAS mutant inhibitors have been linked to a VHL E3 ligase ligand, responsible for recruiting the ubiquitination machinery to mutant KRAS proteins.49,50 These compounds are currently in preclinical development.
T-Cell Immunotherapies
Immunotherapies are also being investigated for targeting RAS-driven cancers because several KRAS mutants are presented as neoantigens – antigens produced specifically by tumor cells and not normal cells – via major histocompatibility complex (MHC) This opens up the possibility of discovering T-cell receptors (TCRs) that target these neoantigens. Tran et al found TCRs expressed in tumor-infiltrating lymphocytes (TILs) that target neoantigens from KRAS G12D mutants.51 Adoptive cell transfer (ACT) of these TILs into patients with KRAS G12D mutant colorectal cancer resulted in regression of pulmonary metastases. Other groups have discovered TCRs that recognize neoantigens derived from KRAS G12V and G12R mutants and demonstrated efficacy in mouse xenograft model of NSCLC.52 Using ACT of these TCR-engineered T-cells, this therapy has entered clinical trials.

Figure 4: Strategies for Indirectly Targeting RAS and Emerging Approaches for Targeting Oncogenic RAS with Immunotherapy. a Targeting key post-transcriptional modifications of RAS protein as well as upstream and downstream factors of RAS signaling have been proved as promising strategies for interfering with RAS activity and exhibiting anti-tumor effects in RAS mutant-driven tumors. Inhibitors targeting the key factors controlling RAS post-translational modifications and membrane trafficking (FTase, PDE6δ), upstream mediators (RTK receptors, SHP2, SOS1/2), and downstream effectors (RAF, MEK, ERK, CDK4/6, PI3K, AKT, mTOR1, AURKA, PLK) are listed. FDA-approved drugs are highlighted in blue, others are still under preclinical or clinical study. b Combination of KRASG12C inhibitors with immune checkpoint blockade and development of bispecific antibodies with T cell engager targeting neoepitopes derived from KRASG12C inhibitor-mediated covalent modification of KRASG12C. This figure was created with BioRender.com. Source: Nature. May 23, 2023;8(212).
Next Steps and New Beginnings in RAS Drug Development
The landscape of drug development for targeting RAS mutations in cancer has witnessed remarkable progress in recent years. What was once 'undruggable' has been drugged, marking a significant breakthrough in the field. While these advancements are promising, challenges persist, particularly in addressing resistance mechanisms and optimizing treatment efficacy. Continued translational research, more advanced, clinically relevant cancer models, and artificial intelligence tools for identifying and testing synergistic treatment combinations may help overcome therapeutic resistance and efficacy challenges in RAS-mutant cancers.
Validate Your KRAS-Targeting Strategy
Using Advanced Cancer Models & Predictive AI to Help Direct Oncology Drug Development & Clinic Research Studies

The latest wave of novel therapies targeting KRAS mutations in cancer continues to shine a spotlight on the inadequacies of traditional preclinical oncology CRO approaches. Understanding the complexities of RAS biology and the RAS signaling pathway in cancer is critical to developing the next wave of therapies for RAS-driven cancers.
Beyond PDX cell lines and subcutaneous mouse models, Certis offers innovative translational approaches for validating your KRAS-targeting strategies. Evaluate your compound’s effect on previously treated tumors through in vitro analysis, test it against immunotherapy-resistant subtypes using in vivo models, or investigate the tumor microenvironment in orthotopic patient-derived xenograft (O-PDX) cancer models. Your IND-enabling studies can be customized to mimic a myriad of clinical scenarios, including prior treatment with specific standard-of-care therapies, radiotherapy via whole body or focal radiation, acquired drug resistance, metastases and immune response.
Only Certis Delivers RAS-Targeted Oncology Intelligence™
Certis Oncology Solutions is the only translational partner that combines the predictive power of cancer artificial intelligence with advanced preclinical models to evaluate efficacy and understand the complex mechanisms of action inherent to drugs that target RAS signaling pathways. Whether your pipeline modality involves T-cell therapies, immune checkpoint inhibitors, CAR-T, combinatory or other novel drug development approaches involving Tumor Infiltrating Lymphocytes (TILs) or neoantigens, Certis Oncology can help you obtain the actionable preclinical data you need to move your RAS-targeted therapeutic program forward. Book a meeting or contact us at busdev@certisoncology.com or 858-988-1033 to discuss your specific oncology drug development needs today.
Attending the 5th Annual RAS-Targeted Drug Development Summit in Boston, September 26-28?

Stop by our exhibit booth and afternoon poster session on Day One of the conference to talk to us about your novel drug development strategies and how we can help validate and accelerate your RAS-targeted compounds. Learn more.
References
- Cox AD et al. Drugging the Undruggable Ras: Mission Possible? Nat Rev Drug Discov. 2014;13(11):828-851.
- Cerami1 E et al. The cBio Cancer Genomics Portal: An Open Platform for Exploring Multidimensional Cancer Genomics Data. Cancer Discov. 2012;2(5):401-404.
- Zehir A et al. Mutational Landscape of Metastatic Cancer Revealed from Prospective Clinical Sequencing of 10,000 Patients. Nat Med. 2017;23(6):703-713.
- AACR Project GENIE: Powering Precision Medicine through an International Consortium. Cancer Discov. 2017;7(8):818-831.
- Prior IA et al. The Frequency of Ras Mutations in Cancer. Cancer Res. 2020;80(14):2969-2974.
- Karnoub AE et al. Ras Oncogenes: Split Personalities. Nat Rev Mol Cell Biol. 2008;9(7):517-531.
- Johnson L et al. K-ras is an Essential Gene in the Mouse with Partial Functional Overlap with N-ras. Genes Dev. 1997;11(19):2468-2481.
- Apolloni A et al. H-ras but Not K-ras Traffics to the Plasma Membrane through the Exocytic Pathway. Mol Cell Biol. 2000;20(7):2475-2487.
- Haigis KM et al. Differential Effects of Oncogenic K-Ras and N-Ras on Proliferation, Differentiation and Tumor Progression in the Colon. Nat Genet. 2008;40(5):600-608.
- Malumbres M et al. RAS Oncogenes: The First 30 Years. Nat Rev Cancer. 2003;3(6):459-465.
- Hall BE et al. The Structural Basis for the Transition from Ras-GTP to Ras-GDP. Proc Natl Acad Sci U S A. 2002;99(19):12138-12142.
- Fernández-Medarde A et al. Ras in Cancer and Developmental Diseases. Genes Cancer. 2011;2(3):344-358.
- Fedele C et al. SHP2 Inhibition Diminishes KRASG12C Cycling and Promotes Tumor Microenvironment Remodeling. J Exp Med. 2020;218(1):e20201414.
- Gebregiworgis T et al. The Q61H Mutation Decouples KRAS from Upstream Regulation and Renders Cancer Cells Resistant to SHP2 Inhibitors. Nat Commun. 2021;12:6274.
- Gimple RC et al. RAS: Striking at the Core of the Oncogenic Circuitry. Front Oncol. 2019;9:965.
- Traut TW. Physiological Concentrations of Purines and Pyrimidines. Mol Cell Biochem. 1994;140(1):1-22.
- Punekar SR et al. The Current State of the Art and Future Trends in RAS-Targeted Cancer Therapies. Nat Rev Clin Oncol. 2022;19(10):637-655.
- Whyte DB et al. K- and N-Ras are Geranylgeranylated in Cells Treated with Farnesyl Protein Transferase Inhibitors. J Biol Chem. 1997;272(22):14459-14464.
- Liu M et al. Targeting the Protein Prenyltransferases Efficiently Reduces Tumor Development in Mice with K-RAS-Induced Lung Cancer. Proc Natl Acad Sci U S A. 2010;107(14):6471-6476.
- Swarthout JT et al. DHHC9 and GCP16 Constitute a Human Protein Fatty Acyltransferase with Specificity for H- and N-Ras. J Biol Chem. 2005;280(35):31141-31148.
- Lai LP et al. Classical RAS Proteins are not Essential for Paradoxical ERK Activation Induced by RAF Inhibitors. Proc Natl Acad Sci. 2022;119(5):e2113491119.
- Song Y et al. Targeting RAS–RAF–MEK–ERK Signaling Pathway in Human Cancer: Current Status in Clinical Trials. Genes Dis. 2022;10(1):76-88.
- Taveras AG et al. Ras Oncoprotein Inhibitors: The Discovery of Potent, Ras Nucleotide Exchange Inhibitors and the Structural Determination of a Drug-Protein Complex. Bioorg Med Chem. 1997;5(1):125-133.
- Herrmann C et al. Sulindac Sulfide Inhibits Ras Signaling. Oncogene. 1998;17(14):1769-1776.
- Ostrem JM et al. K-Ras(G12C) Inhibitors Allosterically Control GTP Affinity and Effector Interactions. Nature. 2013;503(7477):548-551.
- Sotorasib is First KRAS Inhibitor Approved by FDA. NCI website. Published June 25, 2021. Accessed August 21, 2023.
- FDA Grants Accelerated Approval to Adagrasib for KRAS G12C-Mutated NSCLC. FDA website. Published December 12, 2022. Accessed August 21, 2023.
- Dy GK et al. Abstract CT008: Long-term Outcomes with Sotorasib in Pretreated KRASp.G12C-Mutated NSCLC: 2-year Analysis of CodeBreaK100. Cancer Res. 2022;82(12_Supplement):CT008.
- Cannataro VL et al. Heterogeneity and Mutation in KRAS and Associated Oncogenes: Evaluating the Potential for the Evolution of Resistance to Targeting of KRAS G12C. Oncogene. 2018;37(18):2444-2455.
- Zhao Y et al. Diverse Alterations Associated with Resistance to KRAS(G12C) Inhibition. Nature. 2021;599(7886):679-683.
- Koga T et al. KRAS Secondary Mutations That Confer Acquired Resistance to KRAS G12C Inhibitors, Sotorasib and Adagrasib, and Overcoming Strategies: Insights From In Vitro Experiments. J Thorac Oncol Off Publ Int Assoc Study Lung Cancer. 2021;16(8):1321-1332.
- Tripathi R et al. Combating Acquired Resistance to MAPK Inhibitors in Melanoma by Targeting Abl1/2-Mediated Reactivation of MEK/ERK/MYC Signaling. Nat Commun. 2020;11:5463.
- Amodio V et al. EGFR Blockade Reverts Resistance to KRAS G12C Inhibition in Colorectal Cancer. Cancer Discov. 2020;10(8):1129-1139.
- Sun C et al. Intrinsic Resistance to MEK Inhibition in KRAS Mutant Lung and Colon Cancer through Transcriptional Induction of ERBB3. Cell Rep. 2014;7(1):86-93.
- Abstract P05-02: A Phase 1b Study Evaluating the Combination of Sotorasib, a KRASG12C Inhibitor, and Afatinib, a Pan-ErbB Tyrosine Kinase Inhibitor, in Advanced KRAS p.G12C Mutated Non-Small Cell Lung Cancer (NSCLC). American Association for Cancer Research website. Published December 1, 2021. Accessed August 22, 2023.
- Mainardi S et al. SHP2 is Required for Growth of KRAS-Mutant Non-Small-Cell Lung Cancer In Vivo. Nat Med. 2018;24(7):961-967.
- Lou K et al. KRASG12C Inhibition Produces a Driver-Limited State Revealing Collateral Dependencies. Sci Signal. 2019;12(583):eaaw9450.
- Brown WS et al. Overcoming Adaptive Resistance to KRAS and MEK Inhibitors by Co-targeting mTORC1/2 Complexes in Pancreatic Cancer. Cell Rep Med. 2020;1(8):100131.
- dos Santos EO et al. Aurora Kinase Targeting in Lung Cancer Reduces KRAS-Induced Transformation. Mol Cancer. 2016;15:12.
- Hamarsheh S et al. Immune Modulatory Effects of Oncogenic KRAS in Cancer. Nat Commun. 2020;11:5439.
- Tang KH et al. Combined Inhibition of SHP2 and CXCR1/2 Promotes Antitumor T-cell Response in NSCLC. Cancer Discov. 2022;12(1):47-61.
- Canon J et al. The Clinical KRAS(G12C) Inhibitor AMG 510 Drives Anti-Tumour Immunity. Nature. 2019;575(7781):217-223.
- Briere DM et al. The KRASG12C Inhibitor MRTX849 Reconditions the Tumor Immune Microenvironment and Sensitizes Tumors to Checkpoint Inhibitor Therapy. Mol Cancer Ther. 2021;20(6):975-985.
- Wang X et al. Identification of MRTX1133, a Noncovalent, Potent, and Selective KRASG12D Inhibitor. J Med Chem. 2022;65(4):3123-3133.
- Zhang Z et al. GTP-State-Selective Cyclic Peptide Ligands of K-Ras(G12D) Block Its Interaction with Raf. ACS Cent Sci. 2020;6(10):1753-1761.
- Tanaka N et al. Clinical Acquired Resistance to KRASG12C Inhibition Through a Novel KRAS Switch-II Pocket Mutation and Polyclonal Alterations Converging on RAS-MAPK Reactivation. Cancer Discov. 2021;11(8):1913-1922.
- Gustafson WC et al. Direct Targeting of RAS in Pancreatic Ductal Adenocarcinoma with RMC-6236, a First-in-Class, RAS-Selective, Orally Bioavailable, Tri-Complex RASMULTI(ON) Inhibitor. J Clin Oncol. 2022;40(4_suppl):591-591.
- Békés M et al. PROTAC Targeted Protein Degraders: The Past is Prologue. Nat Rev Drug Discov. 2022;21(3):181-200.
- Bond MJ et al. Targeted Degradation of Oncogenic KRASG12C by VHL-Recruiting PROTACs. ACS Cent Sci. 2020;6(8):1367-1375.
- Bery N et al. A Potent KRAS Macromolecule Degrader Specifically Targeting Tumours With Mutant KRAS. Nat Commun. 2020;11:3233.
- Tran E et al. T-Cell Transfer Therapy Targeting Mutant KRAS in Cancer. N Engl J Med. 2016;375(23):2255-2262.
- Bear AS et al. Biochemical and Functional Characterization of Mutant KRAS Epitopes Validates This Oncoprotein for Immunological Targeting. Nat Commun. 2021;12:4365.
ABOUT THE AUTHOR
Elie Diner has a PhD in bioengineering and 12 years of research experience in microbiology, synthetic biology and immunology. During his time at the bench, he developed a passion for effective science communication and eventually transitioned into a career as a professional science and content writer. He's authored 12 peer-reviewed scientific publications and numerous blogs, whitepapers, and eBooks for life science companies.
Back to Feed